Video "Vitamin D: What the Largest Studies Really Show" del canal de youtube MedFacts Daily del doctor John Campbell (Gráfico: Liz Gould)
Transcripción y traducción del video
Bienvenidos al video de hoy. Hoy volveremos a analizar la vitamina D, ya que existen un par de estudios muy convincentes provenientes de Israel, estudios comunitarios a gran escala, basados en la población. Y, una vez más, muestran un patrón consistente.
Las personas con niveles más bajos de vitamina D presentan mayores tasas de infección, mayor número de hospitalizaciones y, según otros estudios, mayor número de ingresos en cuidados intensivos. La evidencia al respecto se acumula cada vez más. Y, para mí, el hecho de que organismos nacionales e internacionales no hayan organizado un ensayo clínico al respecto es casi una negligencia.
La evidencia es tan sólida que realmente necesitamos un ensayo clínico adecuadamente organizado por la Organización Mundial de la Salud, el Servicio Nacional de Salud o los Centros para el Control y la Prevención de Enfermedades, donde sea que estén.
Esto debería hacerse ya. Y el hecho de que no se esté haciendo, en mi opinión, es una negligencia.
En fin, cuatro estudios. El primero es un estudio israelí donde analizaron niveles bajos de vitamina D y descubrieron que esto se asociaba con más casos y más hospitalizaciones. El segundo, un estudio israelí aún más amplio analizó casos positivos y luego descubrió que nuevamente presentaban niveles bajos de vitamina D.
Hicieron lo mismo, pero al revés. Primero analizaron los casos positivos. Luego, al analizarlos, descubrieron que tenían niveles más bajos de vitamina D. Analizaremos algunas directrices estadounidenses y un artículo de revisión.
Ese es el plan para hoy. En resumen, hacemos un llamado a las agencias internacionales para que realicen un ensayo clínico adecuado sobre la vitamina D. Y no hay excusa para no hacerlo.
Realmente debería hacerse.
Pero la evidencia que tenemos ahora es muy sólida, la evidencia de correlación es muy sólida. Ahora, entrando en detalle, el primer estudio israelí... Así que, los niveles bajos de vitamina D en plasma... Así es como se presenta la vitamina D en el plasma.
La 25 OH vitamina D es la vitamina D presente en el plasma. Por lo tanto, cuando es baja, aumentan los casos de COVID19 y el riesgo aumenta. Y, repito, esto es una revisión por pares.
La 25 OH vitamina D es la vitamina D presente en el plasma.
Por lo tanto, cuando es baja, aumentan los casos de COVID19 y el riesgo aumenta.
Y, repito, esto es una revisión por pares.
Este es un estudio publicado. Se habla de la vitamina D como una pandemia mundial. Y, repito, llevamos tiempo hablando de esto.
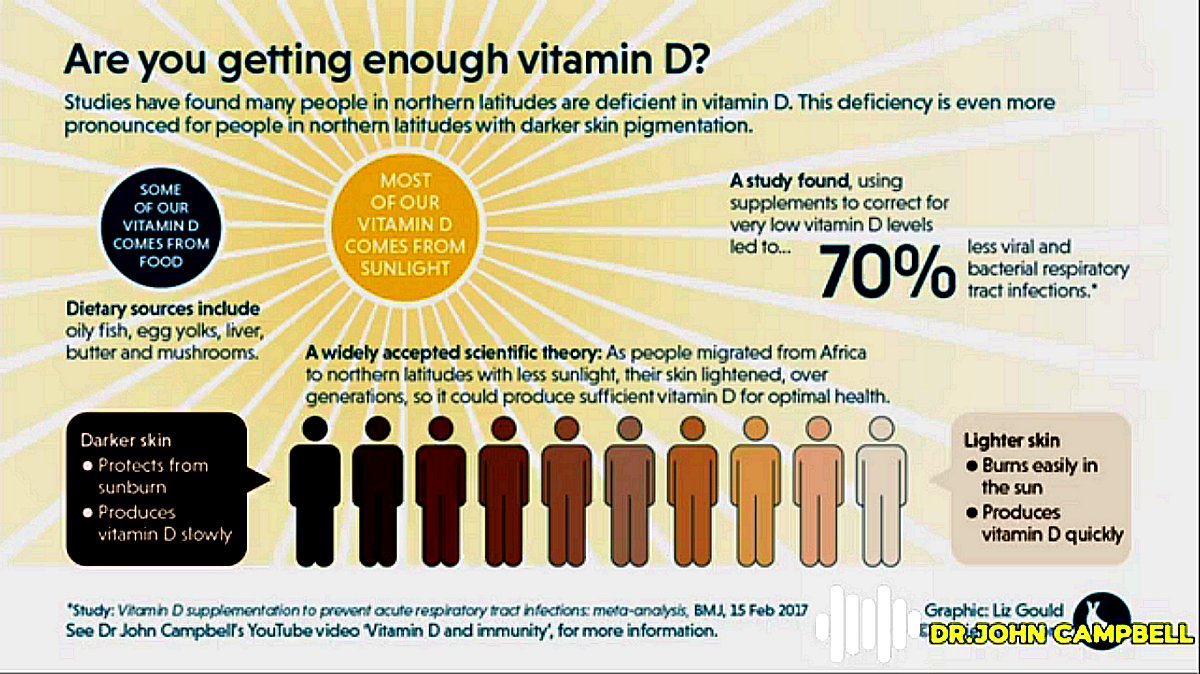
Hemos analizado estudios poblacionales anteriormente y muchas personas presentan deficiencia de vitamina D en todo el mundo. Más del 40 % en Estados Unidos, por ejemplo, presenta deficiencia de vitamina D, con una incidencia mayor en ciertos grupos. Este es un problema global y sabemos desde hace tiempo que está asociado con diversas enfermedades potenciales.
De hecho, las asociaciones son bastante sólidas para varias enfermedades actualmente. Por lo tanto, este estudio buscaba evaluar la asociación entre los niveles plasmáticos de vitamina D y la probabilidad de enfermedad por coronavirus, infección y hospitalización. Comenzaron con un grupo muy grande, pero...
Por lo tanto, este estudio buscaba evaluar la asociación
entre los niveles plasmáticos de vitamina D
y la probabilidad de enfermedad por coronavirus, infección y hospitalización.
Lo bajaron a aproximadamente 7.807 porque ese es el grupo para el cual tenían buena información sobre el estado de la vitamina D.
Como recordarán, los datos se recopilaron entre febrero y abril, y en esa época había muchos casos, y se conocían los niveles sanguíneos de 25 OH vitamina D de los participantes. Eso es positivo. Ahora bien, lo que me gusta de este estudio es que sí definen sus términos.
Siempre es bueno definir términos para que sepamos exactamente de qué estamos hablando.
Ahora dicen que lo subóptimo o bajo es estar por debajo de 30 nanogramos por ml. Entonces lo que están diciendo es que la suficiencia es más de 30 nanogramos por mililitro.
Bueno, si se quiere medir en términos de concentración, como hacemos en el Reino Unido, 70 nanogramos por mililitro equivalen a 75 milimoles por litro. Esos valores son los mismos. Solo que se miden de forma diferente.
La insuficiencia fue de 20 a 30 y la deficiencia fue menor de 20. ¡Qué bajo es todo! Está por debajo del nivel deseado.
Por lo tanto, 30 o más son niveles adecuados. Cualquier valor por debajo de ese nivel es subóptimo o bajo.
Como decimos, buen tamaño de muestra.
Analizaron muchos datos sobre este grupo y descubrieron que el riesgo de ser hombre aumentaba, lo cual coincidía con otros estudios. El riesgo de ser mayor también aumentaba, lo cual coincidía con otros estudios. Sin embargo, descubrieron, y esto empieza a ser coherente con otros estudios, que la obesidad no se asociaba significativamente con un mayor riesgo de infección u hospitalización por COVID19.
Así que los estudios anteriores que mostraban que la obesidad era un factor de riesgo importante ahora plantean algunas dudas.
Y estos datos tampoco lo demostraron. Por lo tanto, todas las demás comorbilidades que analizaron, así como las demás comorbilidades, sí lo fueron, como era de esperar, pero la obesidad no, lo que indica que la obesidad podría no ser un factor de riesgo tan importante como se creía.
Ahora bien, basándose en el tamaño de esa población, de casi 8000 personas, descubrieron que 7000, más de 7000 dieron negativo y casi 800 dieron positivo. Esto realmente proporciona un buen grupo de control.
Entonces, su grupo de control es de 7000 y 25 personas están en su grupo de control.
Y lo que esencialmente tenemos ahí es un grupo experimental, 782.
Entonces, estás comparando a esos con esos. Ese es tu grupo experimental, en realidad, y ese es tu grupo de control.
Entonces dieron negativo, dieron positivo para la enfermedad del coronavirus.
Y, por supuesto, compararon eso con si pertenecían a este grupo, si eran insuficientes o deficientes, o si eran suficientes o no. Así que todo es bastante estándar.
Y lo que encontraron fue una mayor probabilidad de infección por COVID19, de que alguien fuera diagnosticado positivo; la razón de probabilidades fue de 1,45. En otras palabras, las personas con niveles bajos de vitamina D tenían un 45 % más de probabilidades de ser diagnosticadas con COVID19. Pero en cuanto a la hospitalización, las personas con niveles bajos de vitamina D tenían casi el doble de probabilidades de ser hospitalizadas. Tenían un 95 % más de probabilidades de ser hospitalizadas si tenían niveles bajos de vitamina D.
En otras palabras, las personas con niveles bajos de vitamina D tenían un 45 % más de probabilidades de ser diagnosticadas con COVID19.
Pero en cuanto a la hospitalización, las personas con niveles bajos de vitamina D tenían casi el doble de probabilidades de ser hospitalizadas.
Tenían un 95 % más de probabilidades de ser hospitalizadas si tenían niveles bajos de vitamina D.
Las personas con niveles bajos de vitamina D tienen un 45 % más de probabilidades de ser diagnosticadas. Las personas con niveles bajos de vitamina D tienen un 95 % más de probabilidades de ser hospitalizadas. Esto se basa en muestras bastante representativas que comparan estos dos grupos y luego comparan esto con su nivel de vitamina D, independientemente de si pertenecían a este grupo o no.
Es bastante estándar. El grupo empleó técnicas estadísticas bastante sofisticadas, pero todo es bastante estándar. Y concluyeron que los niveles plasmáticos bajos de vitamina D parecen ser un factor de riesgo independiente de infección y hospitalización por COVID19. En otras palabras, es un factor de riesgo independiente.
Lo que querían decir es que, tras considerar otros factores como la hipertensión, las enfermedades pulmonares y cardíacas, encontraron que los niveles bajos de vitamina D eran un factor de riesgo independiente. Esto coincide con muchos otros estudios. Este también es un estudio israelí.
Ahora bien, esto aún no ha sido revisado por pares. Lo he leído y, debo decir, me parece bastante bueno. Parece un estudio bastante bueno.
Así que me complace informarlo. Pero aún no ha sido revisado por pares. Espero que lo sea en una o dos semanas.
Este es un estudio a gran escala en todo Israel. Encontraron 52.000 personas infectadas y aproximadamente medio millón pudieron usarlas como grupo de control. Así que, de nuevo, tenemos dos grupos preparados: ese número de infectados y ese número de no infectados.
Así que nos da cifras muy buenas para comparar y contrastar el estado de vitamina D entre estos dos grupos. No necesito leer los resultados ahora, ¿verdad? Estas fueron sus conclusiones: mayor incidencia de COVID19 con niveles más bajos de vitamina D.
Se está volviendo un poco aburrido, ¿verdad? Mayor incidencia de COVID19 con niveles más bajos de vitamina D. Pero no es aburrido.
Estamos hablando de la vida de las personas.
Pero los mismos resultados se repiten una y otra vez, estudio tras estudio.
Mayor prevalencia de infección con niveles más bajos de vitamina D. Por lo tanto, cuanto más bajos eran los niveles de vitamina D, más probable era que alguien fuera diagnosticado, como si no pudiéramos haberlo previsto.
Efecto protector significativo en quienes tomaron el suplemento durante las cuatro semanas previas. ¡Increíble! Estamos hablando de una encuesta a gran escala.
Y afirman que las personas que tenían niveles bajos de vitamina D previamente, pero que los habían aumentado durante cuatro semanas, tras solo cuatro semanas de suplemento de vitamina D, experimentaron un gran efecto protector contra la COVID19. Esta es una afirmación notablemente significativa. Y cuando investigadores como este dicen significativo, lo que quieren decir es que es estadísticamente significativo.
Y afirman que las personas que tenían niveles bajos de vitamina D previamente, pero que los habían aumentado durante cuatro semanas,
tras solo cuatro semanas de suplemento de vitamina D, experimentaron un gran efecto protector contra la COVID19.
Esta es una afirmación notablemente significativa. Y cuando investigadores como este dicen significativo, lo que quieren decir es que es estadísticamente significativo.
Tienen una seguridad superior al 95%, y de hecho, bastante superior al 95%, de que este resultado es válido. Se observó un efecto protector significativo en quienes habían tomado suplementos de vitamina D durante las cuatro semanas anteriores. Un estudio de gran envergadura.
Eso es lo que dicen las cifras. ¿Es esto una prueba? No. Este es un estudio observacional de correlación a gran escala.
¿Cómo lo demostraríamos? Necesitamos un ensayo clínico aleatorizado, ciego y controlado. ¿Por qué no se lleva a cabo? La evidencia es tan contundente ahora. Como profano, casi diría que está probado, pero científicamente no podemos decirlo porque no tenemos los datos de los ensayos clínicos.
Pero vaya, la evidencia se está acumulando. Ahora, varias organizaciones estadounidenses han elaborado una guía conjunta sobre la vitamina D en la era de la COVID19. Y esta es de la Sociedad Americana para la Investigación Ósea y Mineral.
Éste de aquí, lo he escrito, por cierto, éste de aquí es la Asociación Americana de Endocrinólogos Clínicos, Sociedad Endocrina.
Esta es la Sociedad Europea de Tejidos Calcificados. Dicho de otro modo, se especializan en huesos.
Ésta es la Fundación Nacional de Osteoporosis de Estados Unidos.
Y esta es la Organización Internacional de Osteoporosis. Así que, por supuesto, estos especialistas en neuromuscularidad ósea llevan mucho tiempo estudiando la vitamina D, pero han continuado.
Bueno, eso es justo. Ahora bien, ¿qué dicen? Dedica al menos de 15 a 30 minutos al día a la exposición solar directa, evitando las quemaduras.
Claro, depende del sol, ¿no? La mayoría de los adultos mayores y jóvenes pueden consumir de 40 a 1000 unidades internacionales como suplemento si no reciben suficiente sol.
Si ven el video que hicimos hace un tiempo con Matt, el médico australiano, él dijo que para producir suficiente vitamina D, el sol necesita estar a 45 grados, y depende de la superficie corporal expuesta. Pero dijo que si sales al sol en pantalones cortos en el jardín trasero, recibes un poco de sol por delante y por detrás. Si te expones al sol la mitad del tiempo que tardarías en quemarte, producirás 20.000 unidades internacionales de vitamina D.
Eso es mucho.
Eso es mucho. Así que mis tabletas de 25 microgramos equivalen a mil. Así que, salir al sol sería como tomar 20 de esas tabletas.
Así que es bastante. Ahora bien, también depende de la superficie corporal. Este es mi libro de fisiopatología que escribí hace unos años, y contenía algo llamado la Regla de los Nueve, que se usa para calcular la superficie corporal quemada en personas que sufren quemaduras.
Y lo que significa es que la cabeza representa el 9% de la superficie corporal, un brazo representa el 9% de la parte delantera y trasera, el tronco representa el 18% de la parte delantera y trasera, y las piernas representan el 18% de la superficie corporal. Esto se llama la Regla de los Nueve. Es decir, nueve para un brazo, nueve para un brazo, dieciocho para una pierna, dieciocho para una pierna, dieciocho para la parte delantera, dieciocho para la espalda y nueve para la cadera.
Así que ya ven por qué se llama la Regla del Nueve. No me vieron entonces, pero no importa, lo repetiré. Nueve, 18, nueve, nueve, piernas, 18, 18, espalda, incluyendo los glúteos, 18%.
Para que puedas ver cuánta vitamina D producirás, depende de la proporción de piel expuesta al sol. Así que si puedes tomar un poco de sol, la mitad del tiempo que te quemarás, vas a producir... 20.000 unidades de vitamina D, que es muchísimo. Pero claro, muchos de nosotros no nos exponemos al sol.
Por eso este grupo recomienda que quienes no se exponen al sol puedan tomar este suplemento, aunque sé que recomiendan la dosis baja. Para ser justos, si lo tomas a diario durante años, tus niveles aumentarán y se mantendrán. Sin embargo, muchos tenemos deficiencia de vitamina D, por lo que necesitamos aumentarla un poco. Por eso, son muy conservadores con las dosis.
Ahora, este es el artículo de revisión de The Lancet. Vitamina D y COVID19. ¿El riesgo de deficiencia conlleva un pronóstico más desfavorable para las personas con este riesgo?
Y nuevamente, es un artículo reciente de The Lancet, así que le daremos un vistazo rápido.
Al comparar datos entre países, la mortalidad por COVID19 es claramente mayor en algunos países que en otros. De acuerdo, lo aceptamos. El estado relativo de vitamina D de la población parece medirse, y se ha medido en muchos... casos.
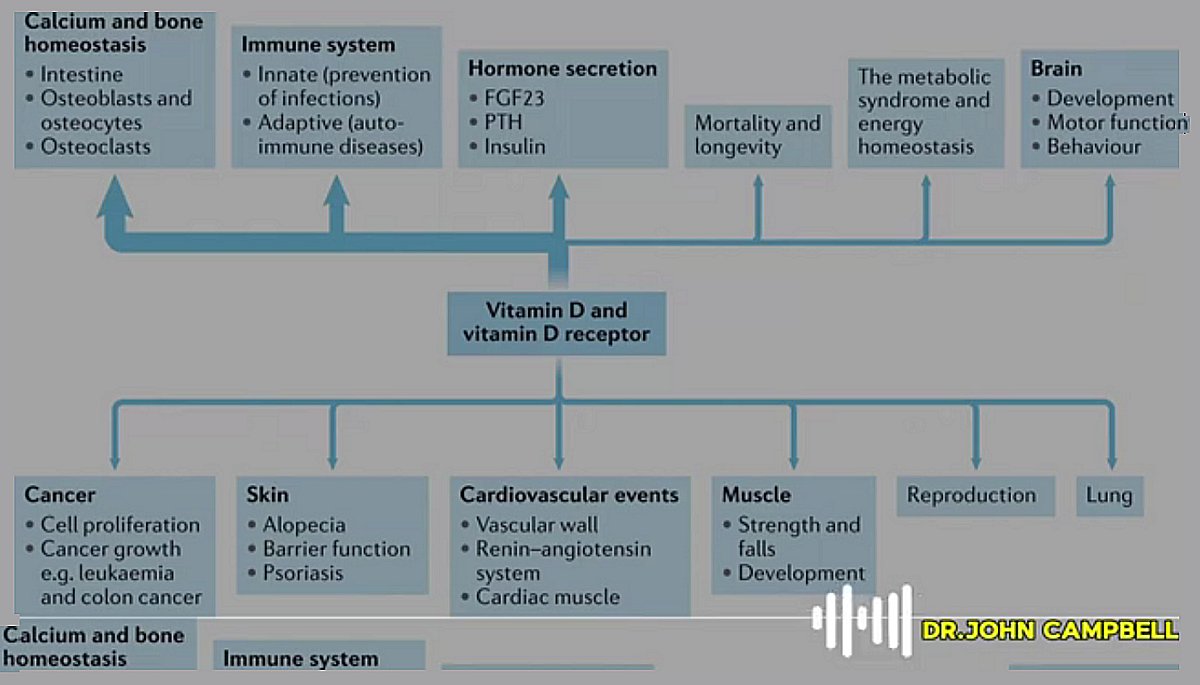
Los suplementos vitamínicos deberían ser especialmente importantes para las personas mayores, en parte porque su piel los produce más lentamente y en parte porque suelen salir menos al aire libre. Las funciones óseas, bueno, las conocemos desde hace siglos. Eso no es nuevo, el raquitismo en los niños... puede causar.
Pero ahora también conocemos muchas otras afecciones, en concreto las infecciones asociadas con una mayor susceptibilidad a las enfermedades infecciosas. Por lo tanto, las personas con niveles bajos de vitamina D son más susceptibles a las enfermedades infecciosas. Numerosos estudios lo indican.
En particular, las infecciones de las vías respiratorias superiores. Tratar los niveles más bajos ofrece el mayor beneficio porcentual. En otras palabras, aumentar los niveles de vitamina D puede ayudar a la mayoría de las personas, pero quienes tienen los niveles más bajos obtendrán el mayor beneficio rápidamente.
En otras palabras, es como una fruta de baja altura, ¿no? Es la más fácil de recoger. Así, las personas con niveles bajos de vitamina D con suplementos recuperan sus niveles rápidamente. Disfrutarán de un gran beneficio de las infecciones de las vías respiratorias superiores rápidamente.
Hablando específicamente de la COVID19, el virus surgió y comenzó a propagarse en el hemisferio norte a finales de 2019. Era invierno y los niveles de vitamina D eran bajos.
Los niveles en sangre son los más bajos. Numerosos estudios epidemiológicos lo demuestran. Los niveles de vitamina D aumentan en verano y disminuyen en invierno a nivel poblacional.
A menudo, cuando suben en verano, no lo suficiente, pero suben. Pero en invierno, bajan. Esto se sabe en varios países y en varios estudios.
La mortalidad por COVID19 se asoció significativamente con el nivel de vitamina D en diferentes poblaciones. Por lo tanto, al analizar diferentes poblaciones, las personas con COVID19 tenían mayor probabilidad de presentar deficiencia de vitamina D. Las personas con COVID19 más grave tenían mayor probabilidad de presentar niveles bajos de vitamina D.
La mortalidad por COVID19 se asoció significativamente con el nivel de vitamina D en diferentes poblaciones.
Por lo tanto, al analizar diferentes poblaciones, las personas con COVID19 tenían mayor probabilidad de presentar deficiencia de vitamina D.
Las personas con COVID19 más grave tenían mayor probabilidad de presentar niveles bajos de vitamina D.
Y sabemos que...
De otros estudios, como el de Indonesia, por ejemplo, se desprende que las personas con niveles bajos de vitamina D eran más propensas a necesitar cuidados intensivos.
Y como aprendimos de los datos de otro ensayo que analizamos hace apenas unos días, la evidencia de esto proviene de todo el mundo.
Es realmente fuerte y acumulable.
Países nórdicos que han tenido buenos resultados, como Suecia, Noruega, Dinamarca y Finlandia. No creo que a los finlandeses les guste que los llamen nórdicos, pero sí a esos países del norte. Pero lo cierto es que Finlandia, Noruega, Suecia y Dinamarca, al estar tan al norte, saben desde hace mucho tiempo, unos diez años, que tienen mucha más probabilidad de sufrir deficiencia de vitamina D que quienes viven más al sur.
Muchos de sus alimentos ya contienen suplementos de vitamina D. Mucha gente lo sabe y toma vitamina D. Por eso, en los países nórdicos, donde las enfermedades graves y las muertes eran menos frecuentes, el nivel de vitamina D es mayor. La evidencia es completamente consistente.
La prevalencia de vitamina D en Italia y España es sorprendentemente común.
Irónicamente, los países nórdicos que no reciben sol lo saben y toman suplementos de vitamina D. Italia y España, que son países soleados, no suplementan su alimentación, pero también tienden a protegerse del sol. Irónicamente, quienes viven en países soleados tienen niveles sorprendentemente bajos.
Sus niveles de deficiencia son sorprendentemente comunes. Sabemos que cuanto más oscura es la piel, más lentamente produce vitamina D. En el Reino Unido, las personas con niveles bajos tienen cuatro veces más probabilidades de morir por COVID19. Además, las minorías étnicas tienen mayor probabilidad de morir.
Sabemos que cuanto más oscura es la piel, más lentamente produce vitamina D.
En el Reino Unido, las personas con niveles bajos tienen cuatro veces más probabilidades de morir por COVID19.
Además, las minorías étnicas tienen mayor probabilidad de morir.
Well, welcome to today's video. And today we're going to be looking at vitamin D again, because there's a couple of very convincing studies have come from Israel, large-scale community, population-based studies. And again, it's showing this consistent pattern.
People with lower levels of vitamin D have higher levels infection, higher levels of hospitalization, and we know from other studies, they have higher levels of admission to intensive care. The evidence for this is just accumulating more and more all the time. And why national and international bodies have not organized a clinical trial on this to me now is getting towards negligence.
The evidence is so strong that we really need a properly organized clinical trial by the World Health Organization or the National Health Service or the Centers for Disease Control, wherever it happens to be. This really should be done now. And the fact that this is not being done in my view is getting negligent.
Anyway, four studies. The first one is an Israeli study where they looked at low levels of vitamin D and they found that that was associated with more cases and more hospitalizations. Second, even larger Israeli study looked at positive cases and then found they had low vitamin D levels again.
So they did the same thing just the other way around. They looked at the positive cases first. Then when they looked at the positive cases, they had lower levels of vitamin D. We're going to look at some US guidelines and we're going to look at a review paper.
So that's the plan for today. So the bottom line is we are calling I am calling on international agencies to do a proper clinical trial on vitamin D. And this really there's no excuse why this shouldn't be done. It really should be done.
But the observation of evidence we have now is so strong, the correlation evidence is so strong. Now, going into the detail, the first Israeli study. So the low plasma vitamin D. So that's the form of vitamin D in the plasma.
The 25 OH vitamin D is the vitamin D in the plasma. So when that's low, the cases of covid-19 are increased, increased risk. And again, this is peer review.
This is a proper published study. So they talk about vitamin D as being a worldwide pandemic. And again, we've been talking about this for some time.
We've looked at population studies before and so many people are deficient in vitamin D around the world. Over 40% in the United States, for example, are vitamin D deficient, higher in certain groupings. This is a global problem and we've known for some time this is associated with quite a few potential diseases.
And in fact, the associations are really quite strong for quite a few diseases now. So this study wanted to evaluate association of plasma vitamin D levels and the likelihood of coronavirus disease, infection and hospitalization. They started off with a very large group, but they've got it down to about 7,807 because that's the group for whom they had good vitamin D status information.
Data was collected, as you might remember, February to April, and there was a lot of cases then and the participants' blood levels of 25 OH vitamin D was known. So that's good. Now, what I like about this study is they do define their terms.
Always nice to define terms so we know exactly what we are talking about. Now, they are saying that suboptimal or low is below 30 nanograms per ml. So what they're saying is that sufficiency is more than 30 nanograms per milliliter.
Well, if you want to measure that in terms of concentration, as we do in the UK, that's 70 nanograms per milliliter is equal to 75 millimoles per liter. Those values are the same. It's just different ways of measuring it.
Insufficiency was 20 to 30 and deficiency was less than 20. So low is anything here. This is below the level that we would want.
So 30 and above is good levels. Anything below that is suboptimal or low. As we say, good sample size.
Now, they did a lot of data on this group and what they found out was that the risks for being male were increased consistent with other studies. The risk for being older were increased consistent with other studies. But what they found out, and this is starting to be consistent with some other studies now, is that obesity was not significantly associated with increased risk for COVID-19 infection or hospitalisation.
So the earlier studies that show that obesity was a big risk factor, there's now a bit of a question mark over those studies. And this data likewise did not show that. So all the other comorbidities they looked at and the other comorbidities were, as you would expect, but the obesity one was not, indicating that obesity may not be as big a risk factor as we had thought.
Now, based on that population size, that nearly 8000 people, what they found out was that 7000, over 7000 tested negative, nearly 800 tested positive. So what that does really is it gives you a nice control group. So your control group there is 7000 and 25 people in your control group.
And then what you've essentially got there is an experimental group, 782. So you are comparing those with those. So that's your experimental group, really, and that's your control group.
So they tested negative, they tested positive for coronavirus disease. And of course, they compared that with whether they were in this group here, insufficient or deficient, and or compared that with whether they were sufficient or not. So all pretty standard stuff.
And what they found was the increased likelihood of COVID-19 infection, of someone being diagnosed positive, the odds ratio was 1.45. In other words, people with low vitamin D levels were 45 percent more likely to be diagnosed with COVID-19. But when it came to hospitalisation, people with low vitamin D levels were nearly twice as likely to be hospitalised. They were 95 percent more likely to be hospitalised if they had low vitamin D levels.
So people with low vitamin D levels, 45 percent more likely to get diagnosed. People with low vitamin D levels, 95 percent, nearly double, more likely to be hospitalised. And this is this is on quite respectable sample sizes comparing these two groups and then comparing that with their vitamin D status, whether they were in this group or whether they were in this group.
So pretty standard, I mean, the group employed some quite sophisticated statistical techniques, but it's all fairly standard stuff. And they concluded that low plasma vitamin D levels appear to be an independent risk factor for COVID-19 infection and hospitalisation. In other words, it's an independent risk factor.
So what they meant was here they had accounted for the other factors like the high blood pressure and the lung disease and the heart disease, but they still found that the low vitamin D levels was an independent risk factor. Consistent with so many other studies. Now, this one also an Israeli study.
Now, this was not yet peer reviewed. I have read it and it looks pretty good to me, I must say. It looks like quite a good study.
So I'm more than happy to report it. But it has not yet been peer reviewed. I expect it will be in the next week or two.
And this is a large scale study all over Israel. They found 52,000 people were infected and about over half a million they were able to use as control. So again, we've got two ready-made groups here, that many infected, that many not infected.
So it gives us really good numbers to compare and contrast the vitamin D status between these two groups. I don't need to read the results now, do I really? These were their conclusions. Greater incidence of COVID-19 with lower vitamin D levels.
It's getting a bit boring, isn't it? Greater incidence of COVID-19 with lower vitamin D levels. But it's not boring. This is people's lives we're talking about.
But the same results are repeated over and over again, study after study. Higher infection prevalence with lowest vitamin D levels. So the lower the vitamin D levels were, the more likely someone was to be diagnosed, as if we couldn't have anticipated that.
Significant protective effect in those who had supplement over the previous four weeks. Wow. We are talking a big scale survey here.
And they are saying that people who had been low of vitamin D before, but had increased it over four weeks, after just four weeks of vitamin D supplement, there was a big protective effect against COVID-19. That is a remarkably significant statement. And when researchers like this say significant, what they mean is it is statistically significant.
They are more than 95% sure, and in quite a lot more than 95% sure, in fact, that this is a valid result. A significant protective effect in those who had supplemented vitamin D over the previous four weeks. Big study.
That's what the numbers are saying. Is this proof? No. This is a large scale correlation observational study.
How would we prove it? We need a randomised blind controlled clinical trial. Why is this not being done? This evidence is so powerful now. I mean, if, you know, as a layperson, I might almost say case proved on this, but scientifically, we can't say that because we don't have the clinical trial data.
But boy, is the evidence accumulating. Now, joint guidance on vitamin D in, now, this is various American groups, joint guidance on vitamin D in the era of Covid. Now, this one here is the American Society for Bone and Mineral Research.
This one here, I've written these down, by the way, this one here is the American Association of Clinical Endocrinologists, Endocrine Society. This one is the European Calcified Tissue Society. In other words, they specialise in bones.
This one is the National Osteoporosis Foundation in the United States. And this one is the International Organisation of Osteoporosis. So these sort of bone neuromuscular type people, of course, have been studying vitamin D for a long time, but they've carried on.
So that's fair enough. Now, what are they saying? Spend at least 15 to 30 minutes with direct sun exposure each day, avoiding sunburn. Of course, it depends on the sun, doesn't it? Most older and younger adults can safely have an intake of 40 to 1000 international units as a supplement if they're not getting enough sun.
Now, if you watch that video a while ago that we did with Matt, the doctor from Australia, he said that to make enough vitamin D, the sun needs to be 45 degrees in the sky, and it depends on the body surface area that's exposed to the sun. But he said if you go out in the sun and you've got your shorts on in your back garden, you get a bit of sun front and back. If you stay in the sun for half of the time it would take you to get sunburned, you'll make 20,000 international units of vitamin D. That's a lot.
That's a lot. So my 25 microgram tablets there, that's equivalent to a thousand. So going out in the sun would be like taking 20 of those tablets.
So it's quite a lot. Now, it also depends on the body surface area. So this is my pathophysiology book I wrote a few years ago, and there was something in there called the Rule of Nine, and this is the Rule of Nine that's used for working out the body surface area that's burnt in people that are burnt.
And what it is, is the head is 9% of the body surface area, an arm is 9% front and back, the trunk is 18% for the front and 18% for the back, and the legs are 18% each of body surface area. So this is called the Rule of Nine. So it's like, so it's like nine for an arm, nine for an arm, 18 for a leg, 18 for a leg, 18 for a front, 18 for a back, nine for a hip.
So you can see why it's called the Rule of Nine. You couldn't see me then, but never mind, I'll do it again. Nine, 18, nine, nine, legs, 18, 18, back, including the buttocks, 18%.
So you can see how much vitamin D you're going to make, depends on the proportion of the skin that is exposed to the sun. So if you can get a bit of sun, half the time to get in sunburned, you're going to make 20,000 units of vitamin D, which is a lot, heck of a lot. But of course, many of us aren't in the sun.
That's why this group is recommending for people that aren't in the sun can take this supplement, but I know they are recommending the low supplement. Now, to be fair, if you are taking this every day for years, that is going to build your level up and it's going to maintain your level if you take it every day for years, but of course, many of us are short of vitamin D, we need to bunk it up a bit. So they're being very conservative in their dosing there.
Now, this is the review article from the Lancet now. Vitamin D and Covid-19. Do deficient risk, do the people at deficient risk a poorer outcome? And again, it's a recent article from the Lancet, so we'll have a quick look through it.
Comparing data across nations, mortality from Covid-19 is clearly higher in some countries than others. OK, we accept that. Relative vitamin D status of the population seems to be measured, has been measured in many cases.
Vitamin supplement should be especially important for older people, partly because their skin makes it more slowly, partly because they often get out into the fresh air less. Functions, well, we've known about the bony functions for ages. That's not new, the rickets in children that it can cause.
But we now know about many other conditions as well, specifically talking about infections associated with increased susceptibility to infectious disease. So people that are low in vitamin D are more susceptible to infectious disease. So many research reports saying that now.
Notably, upper respiratory tract infections. Treating the lowest levels gives most percentage benefit. In other words, putting vitamin D levels up can help most people, but the people with the lowest vitamin D levels will get the most benefit quickly.
In other words, it's kind of like a low-lying fruit, isn't it? It's the easiest to pick. So people with the lowest levels of vitamin D with supplements get their vitamin D levels up quickly. They'll enjoy a lot of benefit from upper respiratory tract infections quickly.
Moving on to Covid-19 specifically. Now, the virus emerged and started to spread in the Northern Hemisphere at the end of 2019. It was wintertime, low vitamin D levels.
The levels in the blood are lowest. We know that's true from numerous epidemiological studies. Vitamin D levels go up in summer, down in winter on a population level.
Very often when they go up in summer, they don't go high enough, but they go up. But in winter, they go down. This is known from multiple countries, multiple studies.
Covid-19 mortality was significantly associated with vitamin D status in different populations. So, again, looking at different populations, people with Covid-19 were more likely to be shortage of vitamin D. People with more serious Covid-19 were more likely to have, the more serious the Covid-19, the more likely it was that their level was low. And we know from other studies, the Indonesian study, for example, that people with low levels of vitamin D were more prone to intensive care.
And as we learned from that other trial data that we looked at just a few days ago. So the evidence for this is really from all over the world now. It really is strong and accumulating.
Nordic countries who have done quite well, so Sweden, Norway, Denmark, Finland. I don't think Finns like being called Nordic, but those northern countries. But what's true is Finland, Norway, Sweden and Denmark, because they're so far north, they've known for quite a long time now, for about 10 years, that they're much more likely to be short of vitamin D than people who live further south.
So a lot of their foods are already supplemented with vitamin D. A lot of the people know about it and a lot of the people take vitamin D. So in the Nordic countries where severe disease and deaths were less common, the vitamin D status is higher. It is all completely consistent evidence. Italy and Spain prevalence of vitamin D is surprisingly common.
So ironically, the Nordic countries that don't get the sun, they know about this and they take extra vitamin D as food supplements. Italy and Spain, which are sunny, they don't supplement their food, but they also tend to keep out the sun. So ironically, these people that live in sunny countries have surprisingly low levels.
Their levels of deficiency are surprisingly common. We know that the darker the coloured skin, the more slowly it produces vitamin D. In the UK, more than four times more likely to die from Covid-19, people with low levels. Well, the ethnic minorities are more likely to die.
And in the States, that was about four point seven percent. And that was from memory from the States, it was about four point seven times increased risk in African-Americans and Indian, American Indians, First Nation Americans. And from memory, I think the risk was about four point six times in Hispanics.
So these are huge, huge differences, huge levels of increased levels of risk because darker coloured skin is making vitamin D more slowly.